Anterior lumbar interbody fusion
(ALIF) Anterior lumbar interbody fusion
(ALIF)
Anterior lumbar interbody fusion, also known as ALIF,
is an
  operation primarily performed for the treatment of low back pain.
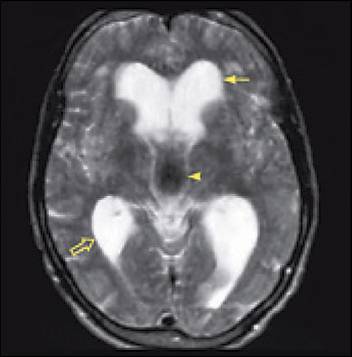
Often, a lumbar discogram is performed. If the
MRI picture showing degeneration of a disk
space matches the level of pain produced during the
discogram, then surgery will have a
good chance of helping the pain. operation primarily performed for the treatment of low back pain.
Often, a lumbar discogram is performed. If the
MRI picture showing degeneration of a disk
space matches the level of pain produced during the
discogram, then surgery will have a
good chance of helping the pain.
This operation is mainly attempting to help low back
pain, although lower extremity pain is occasionally improved, because the
implant into the disk space spreads the vertebral bodies apart, opening the
neural foramen through which the nerve roots leave the spinal canal.
This procedure is not a good option if a patient is
suffering mainly from lower extremity pain because the nerve roots are not
vusialized. A surgery from a posterior approach is a better option.
This may be either a posterior lumbar interbody
fusion (PLIF) or a pedicle screw fixation.
Procedure
  The initial portion (approach) is usually performed by
a vascular surgeon, who exposes the anterior border of the lumbar spine for
the neuro or orthopedic surgeon. The pertinent vascular structures in
this area are the aorta, vena cava, iliac arteries The initial portion (approach) is usually performed by
a vascular surgeon, who exposes the anterior border of the lumbar spine for
the neuro or orthopedic surgeon. The pertinent vascular structures in
this area are the aorta, vena cava, iliac arteries and iliac veins, as well as the pelvic veins. The ureters are also in the vicinity.
Seen here is a typical retractor system, used by the vascular surgeon to
expose the anterior aspect of the spine. In the close us view, visible
are the iliac arteries, and the anterior body of L5. and iliac veins, as well as the pelvic veins. The ureters are also in the vicinity.
Seen here is a typical retractor system, used by the vascular surgeon to
expose the anterior aspect of the spine. In the close us view, visible
are the iliac arteries, and the anterior body of L5.
 

The instruments used for implantation are quite
extensive.
Once the front of the spine is exposed, the surgeon
finds the midline, by using "C arm" (fluoroscopy), which
essentially
provides an x ray in real time. The disk interspace is prepared, and
then the implant is placed within the disk space. The implant may be
a titanium cage (packed with
 cancellous bone from the iliac crest (hip)),
threaded on the outside to prevent backout.
It might also be a threaded cadaver bone dowel, taken from the bone bank.
On the right, two cages are seen from the front, implanted in a translucent
spine model. cancellous bone from the iliac crest (hip)),
threaded on the outside to prevent backout.
It might also be a threaded cadaver bone dowel, taken from the bone bank.
On the right, two cages are seen from the front, implanted in a translucent
spine model.
Often this operation is a stand alone procedure, and
the patient is kept in a lumbar brace for three months postoperatively.
On the other hand, it is occasionally necessary, either early or later on,
to supplement the ALIF with a posterior lumbar fusion using pedicle screws.

The C-arm provides real time imaging to tell the
surgeon where the instruments are.

Anterior lumbar interbody fusion surgery requires a
team effort. Involved in the case are two scrub nurses, a neuro or
orthopedic surgeon, an anesthesiologist, and a C-arm technician.
Complications
Significant complications are not frequent, but they
certainly can occur. There can be complications arising from the
approach to the spine. If there are injuries to any of the great
vessels, significant hemorrhage may occur. The retractors can occlude
the blood supply to the lower extremities. There is a 3-5% risk of
injury to autonomic nerves lying on the front of the spine, resulting in
retrograde ejaculation. Males who intend to have children are given
the option of giving to a sperm bank prior to surgery. There is always
a risk of pushing disk material into the nerves when the disk space is
prepared. |